

Connecting Health Communities
We support cross-sector partnerships to tackle health inequalities.
Introduction
We’ve been facilitating cross-sector partnerships to develop practical responses to local issues for over 18 years. We have enabled groups to reach their most isolated and vulnerable community members, ensuring that services meet local needs.
This page shares our learning about how voluntary organisations and local systems can work together to engage with complexity and achieve change: from co-production in Primary Care Networks (PCNs); to sharing learning across the Integrated Care System (ICS).

How we support cross-sector partnerships
Our offer and aims
What is Connecting Health Communities?
Connecting Health Communities involves activities for a ‘steering group’ and a wider ‘partnership group’ as described below:
- Steering group: Key stakeholders from across the local area, representing the cross-sector group, who (with the support of IVAR facilitators) drive and support the work outside the facilitated sessions. Usually a group of eight or more people, it is important to have the involvement of community leaders and NHS representatives.
- Full partnership/Co-designing days: Involving all interested parties within the local area. The steering group seeks representation from across sectors, as well as community voices to shape and take forward agreed activity. These sessions usually involve around 30-60 people. Workshops are ideally in person; however, they can take place online (e.g. Zoom/Microsoft Teams).
- The Champions Network: A group of cross-sector leaders who want to develop their skills for collaborative and partnership working through peer learning. The overall aim of the Champions Network is to enhance confidence and competence to become system leaders and agents of change. Together, members of the network will share ideas and ways of working, and devise strategies to maintain and build on the practice of collaborative working to support action and sustain change in their areas.
- Local coordinating organisation (LCO): An organisation (or organisations) based locally that support the involvement of communities experiencing health inequalities. The LCO is responsible for cascading information following each co-design/partnership session; and coordinating with other communications leads in the local area to disseminate national learning through their networks. There is a small budget to support these organisations working predominantly at a local level, if money is a barrier to their involvement. The LCO is identified with the facilitator and steering group when the local area conversations begin.
- Community involvement budget: For partnership working to be genuinely cross-sector, we understand that voluntary organisations and people with lived experience need to be able to participate and contribute fully, and be at the forefront of leading action for change. There is a small budget available to help cover attendance costs as well as the time of people who take on a more action-focused role in the area.
Our approach
The model that we use for Connecting Health Communities is built around a deep commitment to listening and collaboration. We aim to address health inequalities by bringing together people with lived experience, charities, the NHS and local authorities to co-design solutions. We involve around 100 people in each area, and we prioritise:
- Building relationships for joint action
We create space for the building blocks of partnership working by:
- Connecting people
- Helping them listen to and understand each other
- Identifying a shared starting point for action; and setting realistic and achievable goals
- Acting as Advocates for the community
Our entry point is to champion, promote and enable the voluntary sector to be a valued and influential partner in health and care design and delivery. We privilege the perspectives and voices of people who are furthest from power in our work.
- Flexibility
We have a core offer that we adapt to work for each area we partner with. We notice when things aren’t working and change our approach to meet the needs and circumstances of local partners.
- Style of facilitation
We take an inclusive, fun and human approach – starting with who is in the room, acknowledging emotions and recognising past challenges. We then use creative methods to facilitate difficult, cross-sector conversations which lead to action. This helps to build capacity locally and is itself an act of influencing the local system, by modelling a collaborative approach to problem-solving.
- Taking responsibility to maintain momentum
We play a convening role, holding the process and bigger picture for the partnership as collaborative working gets underway:
- We ensure that next steps are jointly agreed, and that follow-up actions are picked up.
- We tell the story of the work as it evolves, keeping people energised and motivated.
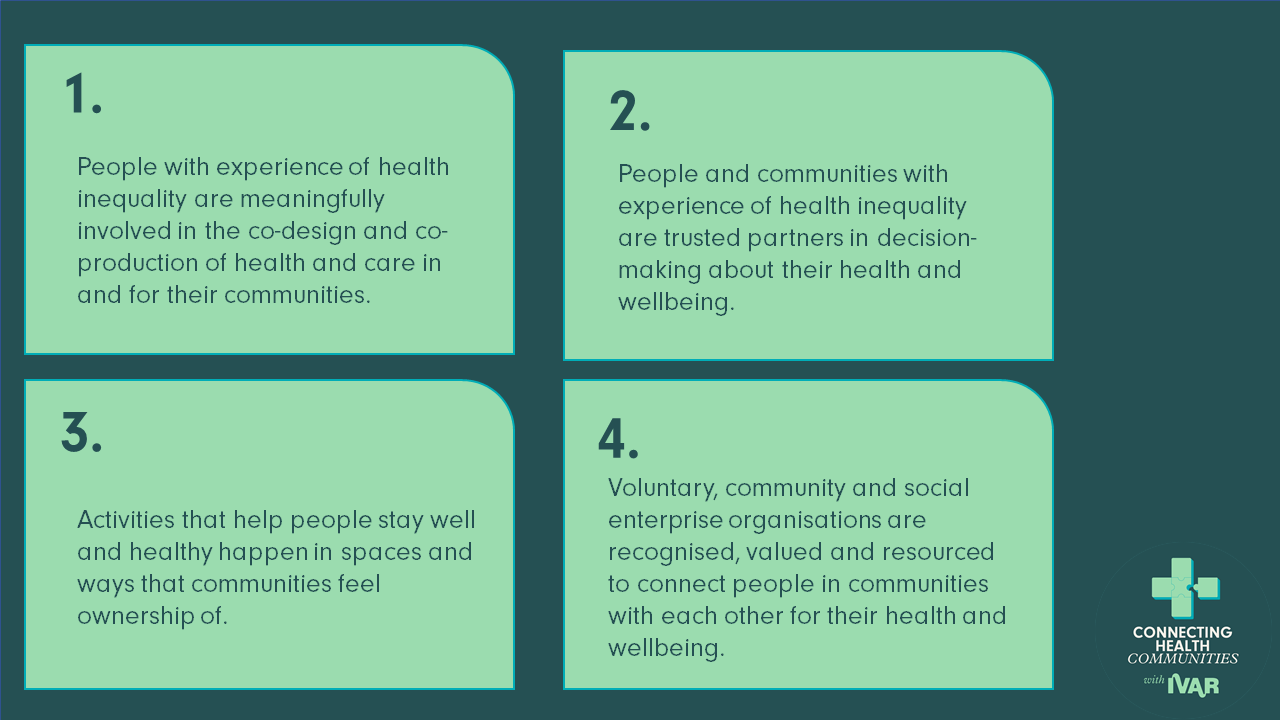
High-level aims
Meet the areas we’re currently working with
We’re currently working with four areas: Barnet & Enfield, Birmingham, East, Dudley, Leicester & Leicestershire and Somerset. Each has a unique health inequality focus.
- Barnet & Enfield aim to enhance access for disabled patients through collaboration among disabled people’s organisations, the voluntary sector, the NHS, and local public health.
- Birmingham aims to strengthen partnerships to address health disparities affecting sex workers, ensuring their voices drive improved healthcare access.
- Leicester & Leicestershire aim to develop a comprehensive homeless health package, bringing together diverse voices and key organisations to explore strategies for effective healthcare delivery.
- Somerset aims to develop a scalable approach to improve discharge experiences for people with dementia, informed by patient, family, caregiver, and health system perspectives.
Challenge, Action, Outcome: Find out more about the aims for each of these areas here.
Resources and learning about…
Know Your Numbers: How Local Action is Preventing Strokes in Cumbria
“What could we do to prevent people having strokes in the first place rather than waiting for them to get ill?”
In 2019, the community of Copeland in West Cumbria faced two urgent challenges: stroke rates that were up to 104% higher than the national average, and difficult changes to local stroke services.
Find out about the Copeland Stroke Prevention Project below…
Case studies
Meet the delivery team
Meet some of the people who help to connect health communities.
We are from the kinds of organisations and communities that we seek to serve. Having worked in and around the voluntary sector as volunteers, paid staff, leaders, trustees, teachers and researchers – we understand and care about the distinctiveness and independence of the sector.

Sonakshi Anand
Programme Manager, Area Lead and Co-facilitator

Keeva Rooney
Area Lead and Co-facilitator
Charlotte Pace
Facilitator

Helen Garforth
Facilitator

Katie Turner
Facilitator and Programme Supervisor

Houda Davis
Area Lead and Co-facilitator

Alexandra Parker
Area Lead and Co-facilitator

Annie Caffyn
Area Lead and Co-facilitator
(on maternity leave)
With thanks to our funder for this work, the National Lottery Community Fund:

You may also be interested in
Listening to what really matters
Four stories of how communities shape health and wellbeing Connecting Health Communities, 2023-25 This…

Better health, together: Four local partnerships in action
From tackling loneliness in St Helens to building trust around TB in Crewe –…

What does it take to build effective solutions and services for our communities?
Building effective health and care solutions or services that address complex community needs and…